Why Do Some Childhood Tumors Resist Treatment? Mitochondria May Provide the Answer, Says Scientist Jan Škoda
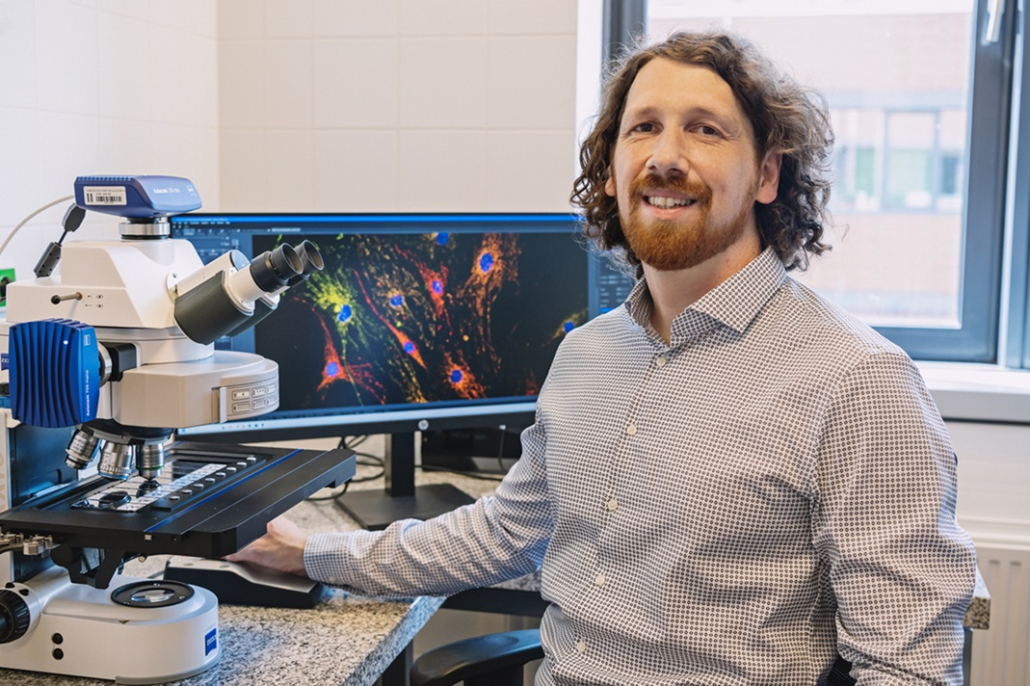
Molecular biologist Jan Škoda studies the hidden world of childhood cancers. He works at the Faculty of Science, Masaryk University, and at the International Clinical Research Center (ICRC) at St. Anne’s University Hospital Brno. In his research, he looks for new ways to overcome tumor resistance to conventional treatments. Working closely with doctors and pathologists, he helps turn lab discoveries into therapies. He has collaborated with leading institutions such as the Children’s Hospital of Philadelphia and the University of Sydney. How might his research improve the way childhood cancers are treated? And could antibiotics one day become part of cancer therapy? These are the questions posed by Jack Barefoot, a Public Relations Intern at ICRC.

Molecular biologist Jan Škoda
Why did you choose oncology as your field of research?
I have always wanted to do research that has a real impact on human health. Even during my undergraduate studies, I was interested in cytogenetics, that studies diseases at the level of abnormalities in our chromosomes, packages of our DNA. It was a field that could be directly applied in hospitals, helping with diagnostics and so on. I was very fortunate to join a group focused on pediatric oncology to work on cytogenetics, but in the context of childhood cancers. My bachelor’s thesis examined how different cytogenetic abnormalities develop when cancer cells are cultured in vitro in the lab—whether they truly reflect what we see in the tumor sample or if they evolve during long-term cultivation in the laboratory.
During this work, I realized that there is so much to study—not only from a diagnostic perspective but, above all, to understand how childhood tumors develop and how we can better target them with treatment. Childhood cancers differ from adult cancers in many ways. Typical adult carcinomas rarely occur in children. Children develop very specific types of tumors that are more closely associated with disruptions in developmental pathways during embryonal development, organ growth, or during growth spurts in puberty. These also overlap with the two peaks of incidence. The first peak is mostly represented by the so-called embryonal tumors, which are common in very young children. The second peak begins to emerge among children older than roughly 12 years, where we are seeing an increase in tumors affecting muscles and bones. Our understanding of their origins is still very limited, and that was exactly my motivation—to identify specific characteristics that are typical of childhood tumors, so that we can treat children with cancer more effectively and with fewer side effects than standard chemotherapy.
How are cancers in children different from those in adult patients?
What sets childhood cancers apart is the way these tumors develop. One of the topics I have focused on is cancer stem cells. We need to understand that not all cancer cells behave the same way—they have different potential to initiate a tumor and drive its aggressive growth. There is a certain hierarchy of this potential, with cancer stem cells at the top. They alone can trigger the entire process of tumor formation.
These cells also share many properties with normal stem cells, which means there is a significant risk that treatment could damage healthy cells along with the cancerous ones. This can have fatal consequences in children.
There are therefore fundamental differences between treating children and adults. Adult patients are typically between 50 and 60 years old, with around 20 years of life ahead of them, so some side effects of treatment are, to some extent, more acceptable in that context… For children, however, similar side effects can dramatically affect their development and future quality of life. Considering this, it is extremely important to explore new treatment options.
„Cancer stem cells also share many properties with normal stem cells, which means there is a significant risk that treatment could damage healthy cells along with the cancerous ones. This can have fatal consequences in children.“
How do you decide which molecules and targets to focus on?
There are different approaches. The first thing that comes to mind is, of course, to focus on molecules that are most abundant in tumor cells compared to healthy cells. This could be a potential target, because tumor cells likely rely on these genes and proteins and therefore overexpress them. You can also focus on targets involved in the regulation of pathways that are mutated. The problem you’re pointing out is that the same proteins can also be overexpressed in other cells or tissues, so this isn’t necessarily a feature unique to the tumor cells. Nowadays, however, there are tools to test this. It’s always important to verify what the normal levels are and how specific receptors or proteins—those we consider as potential targets—are expressed. Naturally, we want treatment to target exactly what makes a tumor cell different from others.
It’s also a good strategy to focus on targets that are broadly present but effective only under certain conditions. That is precisely why I study mitochondria. They are very specific organelles with many important functions in the cell, for example regulating cell death. At the same time, their behavior very often differs between tumor cells and normal cells. We have found that when we target mitochondria—by inhibiting their function— a specific response is triggered. Interestingly, our experiments show that cells from certain cancer types are highly sensitive to this response and rapidly die.
But that must be quite challenging, since mitochondria are present in most human cells…
Yes, but that’s exactly the beauty of this approach! Except for red blood cells, every cell has mitochondria and depends on them for proper functioning. Every cell responds to certain stress signals in the same way. In most cases, it restores homeostasis, meaning balance, and from the perspective of mitochondrial functions, the cell essentially “heals” itself.
However, in tumor cells that overexpress certain oncogenes, this response leads to an excessive reaction that triggers cell death. I think there is a good parallel to why standard chemotherapy is so effective against most, although not all, cancer cells. Chemotherapy targets rapidly dividing cells, which is a very “low-level” mechanism. You’re not targeting one specific signaling pathway, but something so deeply encoded in the cell’s basic physiology that a certain response always occurs.
But the result depends on the circumstances. Since most cancer cells divide quickly, chemotherapy works – at least until they develop some mechanisms of resistance. In our case, if a cell’s dependence on mitochondria is increased by some secondary factor, we can kill it very efficiently, because these factors make the cancer cell selectively vulnerable to the response we induce across mitochondria in all different types of cells.

Jan Škoda during his invited lecture at the St. Anna Children’s Cancer Research Institute in Austria. (Photo: St. Anna Children’s Cancer Research Institute)
Have you discovered why some cancer cells are more sensitive to mitochondrial treatment than others?
There are secondary factors we found to sensitize cancer cells to our mitochondrial treatments. It is a family of similar oncoproteins, proteins that promote uncontrolled cell division when overly active. We are particularly interested in two forms, N-MYC and c-MYC. These forms are highly expressed in very aggressive cases of neuroblastoma, a malignant tumor arising from immature nerve cells that primarily affects infants and children under five. N-MYC was actually first identified in this type of tumor, where it is often amplified, meaning the cell contains numerous copies of the gene encoding this protein. And it is precisely in cases where these MYC factors are amplified that we observe massive cell death after inhibiting mitochondria in our lab. And that is amazing.
Another remarkable aspect is that, to do this, we can reuse some well-tolerated drugs. For example, certain commonly used antibiotics were designed to stop bacteria from making proteins, which they need to survive. Because of their evolutionary origin, mitochondria in our cells are a bit similar to bacteria, so these antibiotics can, to some extent, also inhibit mitochondrial ribosomes – the tiny “factories” that produce proteins inside these organelles. By blocking protein synthesis in this way, we can target the mitochondria in neuroblastoma cells and trigger a reaction that leads to cell death.
If I’m not mistaken, in your work you specifically mentioned doxycycline, a very old antibiotic from the tetracycline group?
Exactly. And I sincerely hope that this idea has the potential to be translated into clinical practice relatively quickly. As part of our new grant, we plan to carry out several studies using animal models and to obtain the highest-quality data possible to support its translation into clinical practice. By this, I mean launching clinical trials and confirming the hypothesis that this is truly something that should be tested across pediatric oncology centers.
The Laboratory Oncology Translational Research Team (ICRC and Faculty of Science, Masaryk University)
Wouldn’t the use of doxycycline and tetracycline antibiotics increase the risk of antibiotic resistance? Especially if they were used in pediatric patients, who may already carry bacteria?
Yes, some resistance can develop. But there are many other classes of antibiotics, so they can later be replaced with different ones if a bacterial infection needs to be treated. However, considering that we are talking about children with cancer, I think the risk that they might later develop resistance to doxycycline is a small price to pay in this situation.
It seems to me that resistance to tetracyclines is fairly common in many bacteria nowadays…
Exactly. Doxycycline is used as a tool to study a wide range of processes. For example, there are doxycycline-regulated gene expression systems, and a great many laboratories work with it. This drug is so commonly used today that I wouldn’t be concerned about contributing to increased resistance to it.
You mentioned that thanks to intensive research in oncology, it is not difficult to obtain the necessary information. But what about funding—is it difficult to secure grants? Especially when we take into account the ongoing wars and other factors that are gradually diverting money away from science?
To be honest, I am personally quite concerned. So far, the situation has been relatively good. You’re right that competition is strong and that funding has always been difficult to obtain, but until now, at least the resources have existed. What will happen next, however, I don’t know… You see, science and culture are always the first areas where cuts are made.
What I think is important to point out is that a great deal of money is invested in oncology research, but research into childhood cancers receives only a tiny fraction of that. And that is something that should change—and hopefully is slowly changing. As I mentioned before, in many respects childhood cancer is essentially a different disease from cancer in adults.
Fortunately, cancers in children are rare—only about 1% of all diagnosed tumors occur in children. However, this also means that we have a limited number of available samples and that there are only a few research groups specializing in childhood tumors. That makes the sharing of samples and new findings between different centers and laboratories extremely important.
The past few years have convinced me that the willingness to collaborate is truly strong. I feel that the motivation to help children drives all of us forward. And that, in my opinion, is what distinguishes childhood cancer research from adult cancer research. In adult oncology, obtaining samples and getting started is much easier, but you have to reckon with very tough competition.
Biologist Karolína Bořánková researches aggressive neuroblastomas in Jan Škoda’s research team. (Photo: Petr Chlapek)
I’ve had a similar personal experience with one laboratory. Research groups working in related areas often see each other as competitors and worry that collaborating might mean losing their ideas. If someone publishes on their topic first, they may find themselves having to start almost from scratch…
There are still people who put their ego above the impact of their work… But as I can tell from a recent conference on childhood cancers, the motivation of pediatric cancer researchers is so strong that they genuinely want to help and are willing to share their materials and ideas with others. And that is incredibly rewarding.
Do you focus mainly on observational or preclinical research, or do you also work on clinical trials? Given how rare childhood cancers are, I would imagine that much of your work falls into the observational category.
Yes, but our research on repurposing drugs to target mitochondria has the potential to develop into a clinical trial. At that stage, it would be the role of pediatric oncologists to implement the idea. To test whether a drug is effective, we start with models. As we collaborate closely with the pediatric oncology department in Brno, we have the opportunity to work with patient-derived models. From patient samples, we derive cell lines that largely retain the biological characteristics of the patient’s tumor. We can then inject these tumor cells into immunodeficient animal models, and monitor tumor development and its response to treatment in real time.
Such models may also open the door to personalized medicine. In practice, we could take a patient’s tumor cells and test them in the lab to see how they respond to different drugs. Based on these results, doctors could then choose the treatment that’s most likely to work best for that individual patient.
Scientists led by Jan Škoda investigate why some cancers resist treatment and seek new ways to overcome this resistance.
Do you also work on relapsing tumors, that is, tumors that repeatedly return in patients? Have you observed that this type of tumor is more resistant to treatment?
Exactly. As part of our collaboration with researchers from the USA, we published a study focusing specifically on cancer resistance mechanisms. It is known that after a relapse, tumor cells are resistant not only to the treatment originally used, but also to other drugs. These patients have then very limited options and their prognosis is usually very poor. We found a new mechanism of resistance that arises directly at the level of mitochondria. Mitochondria play a key role in deciding whether a tumor cell dies in response to therapy. When a patient’s tumor returns, the mitochondria in those tumor cells are no longer sensitive to cell death signals, allowing the cancer cells to evade therapy and survive. As a result, we decided to target treatment directly at the mitochondria, which led us to the previously mentioned ribosomal antibiotics, including doxycycline, and subsequently to studying the relevant pathways, through which we uncovered the mechanism underlying sensitivity to this type of drug.
“We found that some resistance mechanisms arise at the level of mitochondria. Mitochondria play a key role in determining whether controlled cell death occurs.”
How would you explain to a layperson why it’s worthwhile to invest in science?
I think it’s much easier to convince people of the importance of applied research, because its concrete impacts can be shown fairly clearly. It’s much harder, however, to raise awareness of why basic research is important. Yet everything we see around us today stems from ideas built on basic research. Without science, none of what we have today would exist. Modern society is built on technological progress.
The advances we’ve made in health, the increase in average life expectancy, and the improvement in quality of life are easy to measure and demonstrate—and it is science that enabled these developments, from new treatments for diseases to all these gadgets that make our daily lives easier. Without science, we wouldn’t be able to do any of the things we take for granted today. Even the very ability to focus on something, think critically, and try to understand how things work shapes who we are. If you look at it from the ground up, curiosity and the drive to explore and move forward—that is what science is all about.
Author: Jack Barefoot